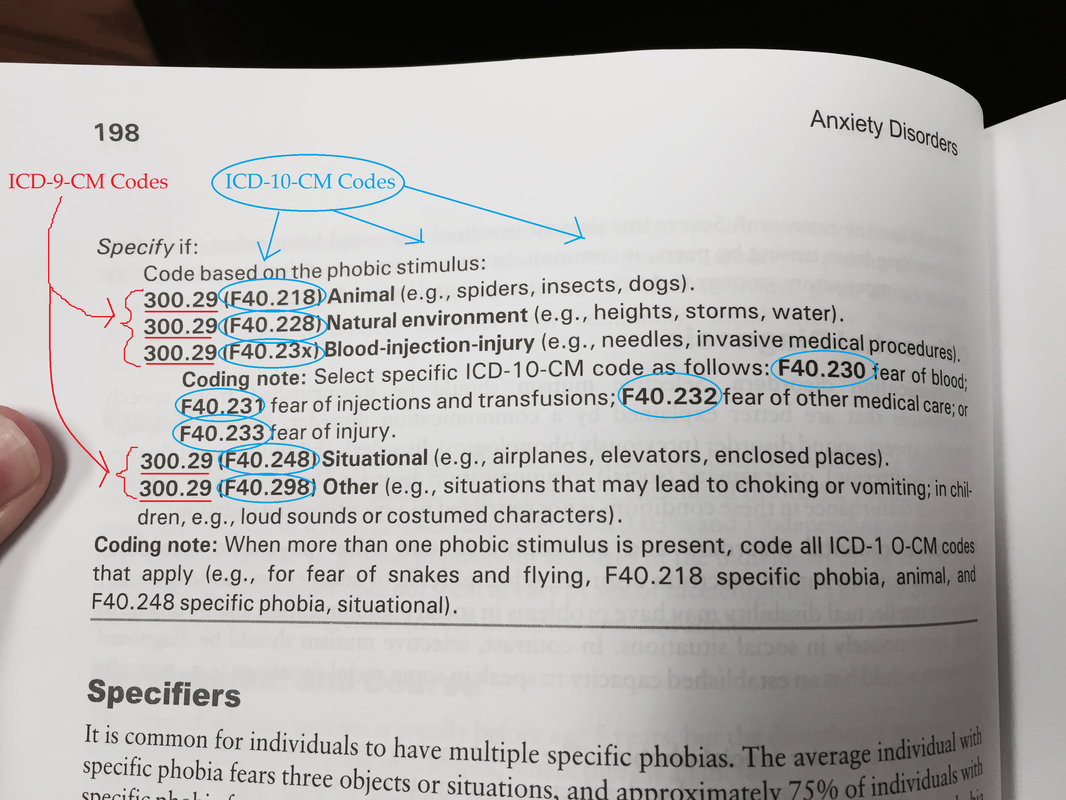
ICD-10 is the International Classification of Diseases (10th Edition). ICD has been published for over a century by the World Health Organization (WHO). ICD-10 differs substantially from ICD-9 in increasing the number of codes (from about 13,000 codes to about 68,000 codes) and increasing the specificity of information indicated by the code—particularly for medicine. The changes are relatively less exponential, but still very important, for behavioral health (for example: specific phobias used to be just one ICD-9 code, 300.29, but now, in ICD-10, you have to specify if the phobia is tied to an animal such as a spider, insect, or dog, F40.218; the natural environment such as heights, storms, or water, F40.228; situations such as airplanes, elevators, enclosed spaces, F40.248; and a couple of other options).
ICD-10 was endorsed in 1990, and implemented internationally by WHO member states in 1994. Almost 100 other countries are using it, but the United States has been behind the times, until now…
In the United States, starting October 1, 2015, based on date of service for outpatient care (or the date of discharge for inpatient care), claims will need to be billed on ICD-10. (Services rendered on September 30, 2015 will continue to be billed/appealed with ICD-9 codes.) (You may remember that this implementation date has been delayed two times previously – from October 1, 2013, and then from October 1, 2014.) We don’t expect delays this time, but the history of delays is important: we’re in a setting in which it feels like someone has cried wolf a couple of times already; payer implementation budgets for training providers have been exhausted already in past years—to the tune of billions spent across the healthcare industry; and yet, all players in the system (payers, EHRs, Clearinghouses, clinicians, and administrative staff) need to be ready as if they weren’t told to hurry up and wait a couple of times already.
To be ready for October 1, 2015, behavioral health providers that accept third party reimbursement need to have DSM-5 diagnoses ready for all active clients. The DSM-5, published in May of 2013, also differs significantly from the DSM-IV-TR (published in 2000, revising the DSM-IV, published in 1994).
The DSM-5, which makes a big conceptual shift from categorical diagnosis to a dimensional model for diagnosis, was designed to match much better with ICD-10. The ICD-10 code can be referenced in multiple ways within the DSM-5 book. For instance, there are three indexes, from pages 839 to 896 of the DSM-5, including one alphabetical index, and two numerical indexes (one is ICD-9 and one is ICD-10). In addition, the ICD-10 code is indicated in parentheses next to the ICD-9 code if there is a one-to-one match. As in our example of a specific phobia above, there is not always a one-to-one match, and a client essentially needs to be “re-diagnosed” with the level of specificity, or conceptual change in the diagnosis, requisite in the DSM-5 for ICD-10 billing purposes.
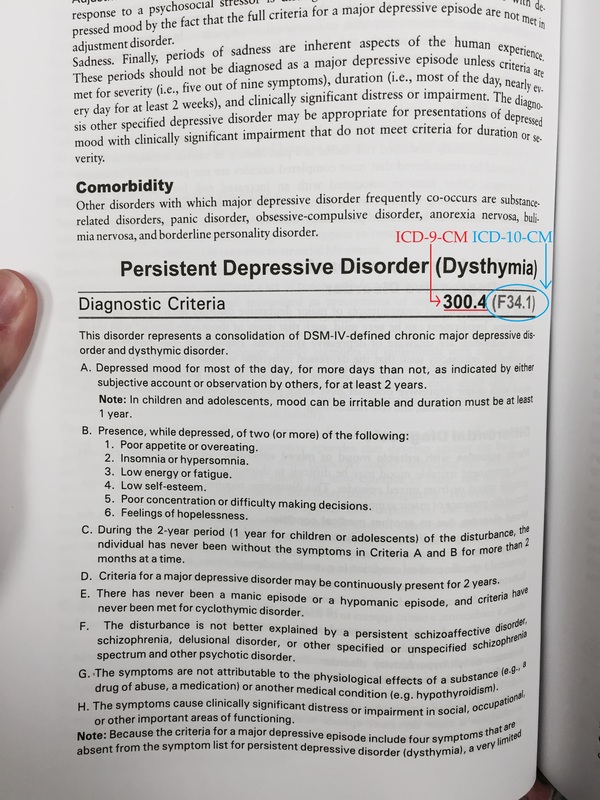
When only one ICD-10-CM is assigned to a disorder, it is at the top of the criteria box:
ICD-10 was endorsed in 1990, and implemented internationally by WHO member states in 1994. Almost 100 other countries are using it, but the United States has been behind the times, until now…
In the United States, starting October 1, 2015, based on date of service for outpatient care (or the date of discharge for inpatient care), claims will need to be billed on ICD-10. (Services rendered on September 30, 2015 will continue to be billed/appealed with ICD-9 codes.) (You may remember that this implementation date has been delayed two times previously – from October 1, 2013, and then from October 1, 2014.) We don’t expect delays this time, but the history of delays is important: we’re in a setting in which it feels like someone has cried wolf a couple of times already; payer implementation budgets for training providers have been exhausted already in past years—to the tune of billions spent across the healthcare industry; and yet, all players in the system (payers, EHRs, Clearinghouses, clinicians, and administrative staff) need to be ready as if they weren’t told to hurry up and wait a couple of times already.
To be ready for October 1, 2015, behavioral health providers that accept third party reimbursement need to have DSM-5 diagnoses ready for all active clients. The DSM-5, published in May of 2013, also differs significantly from the DSM-IV-TR (published in 2000, revising the DSM-IV, published in 1994).
The DSM-5, which makes a big conceptual shift from categorical diagnosis to a dimensional model for diagnosis, was designed to match much better with ICD-10. The ICD-10 code can be referenced in multiple ways within the DSM-5 book. For instance, there are three indexes, from pages 839 to 896 of the DSM-5, including one alphabetical index, and two numerical indexes (one is ICD-9 and one is ICD-10). In addition, the ICD-10 code is indicated in parentheses next to the ICD-9 code if there is a one-to-one match. As in our example of a specific phobia above, there is not always a one-to-one match, and a client essentially needs to be “re-diagnosed” with the level of specificity, or conceptual change in the diagnosis, requisite in the DSM-5 for ICD-10 billing purposes.
When only one ICD-10-CM is assigned to a disorder, it is at the top of the criteria box:
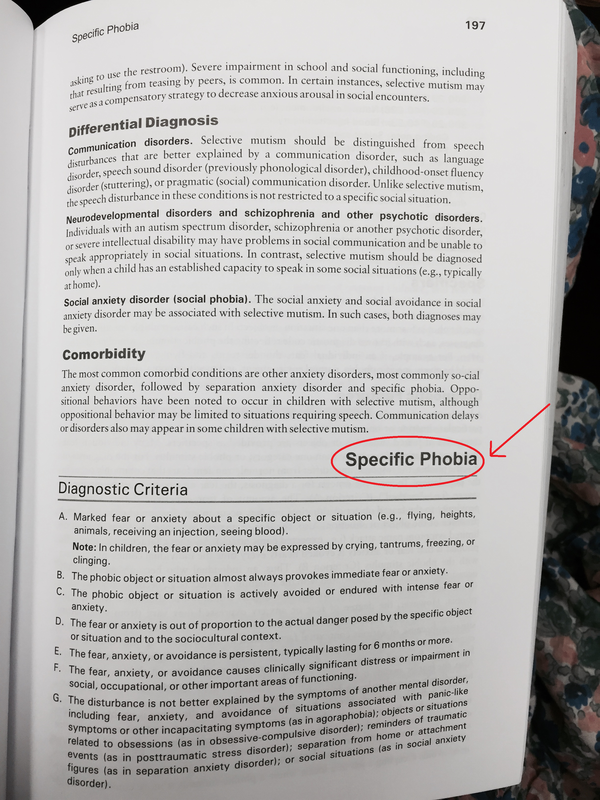
If more than one code can be assigned to a disorder, the codes are at the bottom of the diagnostic criteria box:
 |  |
For various reasons, what is called “dual-coding” is recommended for at least a couple of months before the October 1, 2015 implementation date. In behavioral health, dual-coding really means dual-diagnosing: that clinicians will include the DSM-IV-TR diagnosis (and corresponding ICD-9 code) AND the DSM-5 diagnosis (and corresponding ICD-10 code) in all internal notes for each client. One reason for starting this 2-3 months in advance of October 1 is that not all clients in your system present for therapy weekly. It is also time-consuming to essentially “re-diagnose” your clients, becoming more specific with the DSM-5 diagnoses in some cases. While this goes without saying, we’ll say it anyway: as a clinician, diagnosing is a serious ethical professional responsibility – so re-diagnosing clients needs to be done with care. Your diagnosis will need to be supported with correct documentation, that supports the diagnosis, and in case you are audited for services rendered on or after October 1st, the auditor should find documentation to match the DSM-5 diagnosis/ICD-10 code. This takes time to master.
When dual-diagnosing, you may need to coordinate with IT to be sure there are fields for this, and either follow or encourage the development of an agency policy so that this process is as standardized as possible. The term “dual-coding” might sound like a billing responsibility rather than a behavioral health clinician responsibility. This is because “coding” in the medical community (their billing professional’s responsibility) does often involve reading the physician notes and selecting the right code. Behavioral health billing does not work this way – the code is input, based on the diagnosis, by the treating clinician. (All of the number/letter combos you see in the DSM-5 are from the ICD-9 and/or ICD-10.)
Clinicians that accept third party funding cannot ethically continue to diagnose with DSM-IV-TR diagnoses and expect the billing staff to make “clinical” decisions to convert that diagnosis to a billable ICD-10 code. Because clients do not always come weekly to treatment, and to prevent a general bottleneck of to do’s starting October 1st, the dual-diagnosing/dual-coding needs to start now. That said, you need to follow your agency’s diagnostic policies, and/or state and federal regulations if you are subject to them. After October 1st, it might not be a bad idea to continue to include the DSM-IV-TR diagnosis somewhere in the notes secondary to the DSM-5 diagnosis, because your billing staff may need to haggle with and explain these things to third party payers, etc. #justsaying
There are things we can control, and things we cannot control.
Controllable:
Not controllable:
PS Since your documentation starting on October 1, 2015, needs to match the DSM-5 diagnostic criteria, it’s probably time to get a purple book?:
When dual-diagnosing, you may need to coordinate with IT to be sure there are fields for this, and either follow or encourage the development of an agency policy so that this process is as standardized as possible. The term “dual-coding” might sound like a billing responsibility rather than a behavioral health clinician responsibility. This is because “coding” in the medical community (their billing professional’s responsibility) does often involve reading the physician notes and selecting the right code. Behavioral health billing does not work this way – the code is input, based on the diagnosis, by the treating clinician. (All of the number/letter combos you see in the DSM-5 are from the ICD-9 and/or ICD-10.)
Clinicians that accept third party funding cannot ethically continue to diagnose with DSM-IV-TR diagnoses and expect the billing staff to make “clinical” decisions to convert that diagnosis to a billable ICD-10 code. Because clients do not always come weekly to treatment, and to prevent a general bottleneck of to do’s starting October 1st, the dual-diagnosing/dual-coding needs to start now. That said, you need to follow your agency’s diagnostic policies, and/or state and federal regulations if you are subject to them. After October 1st, it might not be a bad idea to continue to include the DSM-IV-TR diagnosis somewhere in the notes secondary to the DSM-5 diagnosis, because your billing staff may need to haggle with and explain these things to third party payers, etc. #justsaying
There are things we can control, and things we cannot control.
Controllable:
- Training and agency policies, regarding diagnosing with DSM-5, in place before October 1, 2015.
- Dual-coding/dual-diagnosing in practice for a couple of months before October 1, 2015.
- Financial reserves saved in case of delay in payments on October 1, 2015.
- Contact all your health IT vendors, including your electronic health record system (EHR) if applicable, your clearinghouse, and/or your database management system, to be sure that there are fields that allow you to enter the DSM-5 diagnosis and ICD-10 code as well as the DSM-IV-TR diagnosis and ICD-9 code.
- You can ask about provider training from health plans with which you are in-network.
- You can speak with the health plan, make as good of friends as possible with your provider representative, and put him/her on speed dial in advance of October 1st.
- You can budget extra staff time for prior-authorizations, for keying the new codes, for advocating to health plans when inevitably one of the many new codes is not loaded in the system correctly, and for appealing denied claims within the timely filing window after October 1, 2015 and before January 1, 2016.
- You can budget extra staff time to scrupulously review incoming funds to identify and resolve payment issues.
- You can assess the risk by looking at the share of third party funding in your agency budget: is it 12%? Then maybe have a 12% of your budget cushion lined up to cover you for a few months.
- Within third party funding, you can know your payer mix (what plans are the biggest share of your income) and triage strengthening those relationships/having a plan in place for resolving denied claims.
- Have any current billing/claims issues resolved before October 1st, so they don’t get backlogged.
Not controllable:
- Guaranteeing that all codes are loaded correctly by 3rd party payers – will have to watch and advocate fixes for any denied claims as they arise.
- Unlikely to be controllable to 100% avoid some delays in payment—as the system is likely to be overwhelmed by all the changes and corrections to them.
- What other parties do (but you can have the relationships in place to help you resolve the issues/problems as they become apparent).
PS Since your documentation starting on October 1, 2015, needs to match the DSM-5 diagnostic criteria, it’s probably time to get a purple book?:
So you wanna diagnose with DSM-5? This is a non-exhaustive list of some changes to be aware of:
PPS In addition to getting familiar with new DSM-5 diagnostic criteria, it is not so bad to learn more about where the ICD-10 codes come from and how they are organized. (The DSM-5 book already maps to the ICD-10 codes for you, but taking an hour to review Chapter V of the actual ICD-10 book, where most behavioral health codes live, is a quick way to feel a little more informed/authoritative and therefore, if that generally works for you, a little less disgruntled about all of this.) In addition to DSM-5 training, we recommend for you to complete the “Chapter V—Mental and behavioral disorders” (Codes: F00-F99) module in this free World Health Organization ICD-10 training: http://apps.who.int/classifications/apps/icd/icd10training/. It says it takes 80 minutes to complete, but just spending 20 minutes dipping your toe in is likely to provide some benefit and bearings. Do take the time to complete the quizzes at the end, which give more information. A basic overview of the layout of the ICD-10 book, broken into code “blocks,” from Chapter V, which focuses on “Mental and behavioral disorders:”
Code Block Included Diagnoses
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC.
American Psychiatric Association (2013), “Highlights of Changes from DSM-IV-TR to DSM-5.” Link: http://www.dsm5.org/Documents/changes%20from%20dsm-iv-tr%20to%20dsm-5.pdf
American Psychiatric Association (2013), “Insurance Implications of DSM-5.” Link: http://r.search.yahoo.com/_ylt=AwrTHQhrTKBVYg0AXm1XNyoA;_ylu=X3oDMTExYWt2Nmx0BGNvbG8DZ3ExBHBvcwMxBHZ0aWQDVUlDMl8xBHNlYwNzcg--/RV=2/RE=1436597484/RO=10/RU=http%3a%2f%2fwww.psychiatry.org%2fFile%2520Library%2fPractice%2fDSM%2fDSM-5%2fInsurance-Implications-of-DSM-5.pdf/RK=0/RS=U8O44dDcb2Fr7s0tQVjunN_btDg-.
American Psychiatric Association (2014), “Coding Update: Supplement to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.” Link: http://www.omh.ny.gov/omhweb/resources/providers/dsm-5-coding-update.pdf.
American Psychiatric Association (2014), “Understanding ICD-10-CM and DSM-5: A Quick Guide for Psychiatrists and Other Mental Health Clinicians.” Link: http://www.psychiatry.org/home/search-results?k=understanding icd
Carr, J. (2015). The DSM-5: Clinical Assessment, Diagnosis, and Supervision. [PowerPoint]. Presented in Houston, Texas, on March 27, 2015, and June 5, 2015, for the Network of Behavioral Health Providers through the Greater Houston Behavioral Health Affordable Care Act (BHACA) Initiative.
World Health Organization (2010). “ICD-10 Training Tool,” particularly “Chapter V—Mental and behavioral disorders” (Codes: F00-F99). Link: http://apps.who.int/classifications/apps/icd/icd10training/.
- Shift from categorical model to dimensional model
- More specificity
- Substance abuse, etc., is now called substance use
- State of substance use (withdrawal, acute, etc.) is specified
- Section 2 of DSM-5 (containing diagnoses and all the diagnostic criteria) is organized by the human lifetime—with behavioral health issues presenting in childhood coming in the earlier chapters, and behavioral health issues more typical of older age coming in the later chapters
- No more axes
- Instead of axes, you are encouraged to diagnose/code multiple diagnoses
- The reason for presentation and/or admission is most often the primary diagnosis (in some exceptional cases, the longstanding diagnosis might be the primary diagnosis, such as in the case of acute anxiety presenting in someone with long-term schizophrenia)
- Sex differences have been considered in the diagnoses
- What were coded as ICD-9-CM “V codes” have become ICD-10-CM “Z codes.” These are not approved as official diagnosis codes, “but can provide additional context for a clinical formulation and treatment plan,” (American Psychiatric Association, 2013). Examples of Z codes are: “Parent-Child Relational Problem,” “Relationship Distress With Spouse or Intimate Partner,” “Child Psychological Abuse, Confirmed,” etc.
PPS In addition to getting familiar with new DSM-5 diagnostic criteria, it is not so bad to learn more about where the ICD-10 codes come from and how they are organized. (The DSM-5 book already maps to the ICD-10 codes for you, but taking an hour to review Chapter V of the actual ICD-10 book, where most behavioral health codes live, is a quick way to feel a little more informed/authoritative and therefore, if that generally works for you, a little less disgruntled about all of this.) In addition to DSM-5 training, we recommend for you to complete the “Chapter V—Mental and behavioral disorders” (Codes: F00-F99) module in this free World Health Organization ICD-10 training: http://apps.who.int/classifications/apps/icd/icd10training/. It says it takes 80 minutes to complete, but just spending 20 minutes dipping your toe in is likely to provide some benefit and bearings. Do take the time to complete the quizzes at the end, which give more information. A basic overview of the layout of the ICD-10 book, broken into code “blocks,” from Chapter V, which focuses on “Mental and behavioral disorders:”
Code Block Included Diagnoses
- F00-F09 Organic, including symptomatic, mental disorders
- F10-F19 Mental and behavioral disorders due to psychoactive substance use
- F20-F29 Schizophrenia, schizotypal and delusional disorders
- F30-F39 Mood (affective) disorders
- F40-F48 Neurotic, stress-related and somatoform disorders
- F50-F59 Behavioral syndromes associated with physiological disturbances and
physical factors - F60-F69 Disorders of adult personality and behavior
- F70-F79 Mental retardation
- F80-F89 Disorders of psychological development
- F90-F98 Behavioral and emotional disorders with onset usually occurring in childhood
and adolescence - F99 Unspecified mental disorder
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC.
American Psychiatric Association (2013), “Highlights of Changes from DSM-IV-TR to DSM-5.” Link: http://www.dsm5.org/Documents/changes%20from%20dsm-iv-tr%20to%20dsm-5.pdf
American Psychiatric Association (2013), “Insurance Implications of DSM-5.” Link: http://r.search.yahoo.com/_ylt=AwrTHQhrTKBVYg0AXm1XNyoA;_ylu=X3oDMTExYWt2Nmx0BGNvbG8DZ3ExBHBvcwMxBHZ0aWQDVUlDMl8xBHNlYwNzcg--/RV=2/RE=1436597484/RO=10/RU=http%3a%2f%2fwww.psychiatry.org%2fFile%2520Library%2fPractice%2fDSM%2fDSM-5%2fInsurance-Implications-of-DSM-5.pdf/RK=0/RS=U8O44dDcb2Fr7s0tQVjunN_btDg-.
American Psychiatric Association (2014), “Coding Update: Supplement to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.” Link: http://www.omh.ny.gov/omhweb/resources/providers/dsm-5-coding-update.pdf.
American Psychiatric Association (2014), “Understanding ICD-10-CM and DSM-5: A Quick Guide for Psychiatrists and Other Mental Health Clinicians.” Link: http://www.psychiatry.org/home/search-results?k=understanding icd
Carr, J. (2015). The DSM-5: Clinical Assessment, Diagnosis, and Supervision. [PowerPoint]. Presented in Houston, Texas, on March 27, 2015, and June 5, 2015, for the Network of Behavioral Health Providers through the Greater Houston Behavioral Health Affordable Care Act (BHACA) Initiative.
World Health Organization (2010). “ICD-10 Training Tool,” particularly “Chapter V—Mental and behavioral disorders” (Codes: F00-F99). Link: http://apps.who.int/classifications/apps/icd/icd10training/.
 RSS Feed
RSS Feed
